|
DIAGNOSTICS, SAMPLING AND
STUDY
Blastomycosis (North American Blastomycosis)
Blastomycosis is
usually a severe disease, principally of the dog and human (rarely the cat and
other animals), caused by the fungus Blastomyces dermatitidis and
characterized by an infection that usually begins with the formation of
granulomatous nodules in the lungs.
The infection may be confined to the
lungs and regional lymph nodes or metastasize to produce the disseminated
disease with involvement of the skin, bone and other tissues and
organs.
Although there are usually numerous nodules in the lungs, in some
instances metastases may come from very limited pulmonary involvement.
Occasionally the infection is confined to lesions involving the skin and
subcutis. Such infections may persist for
months.
Etiology/Source - Blastomyces dermatitidis is
a soil-borne, dimorphic fungus. The mycelial phase occurs in nature and the
yeast form in vivo.
Distribution/Occurrence - It is probably
worldwide in distribution, although the number of cases reported outside of
North America is relatively small. The endemic area in the United States
includes the middle western, southeastern and Appalachian states. Although
single cases are most frequent, multiple cases have been reported in hunting
dogs.
Susceptibility - The disease occurs most frequently in
dogs; it is rare in cats. Humans are susceptible.
Mode of
Infection/Transmission - Inhalation of spores. Infrequently via
skin wounds leading to cutaneous lesions. Most often cutaneous lesions are
derived from pulmonary infection.
Incubation
Period/Course - . The incubation period is variable and may be as
long as several months. The course likewise is variable.
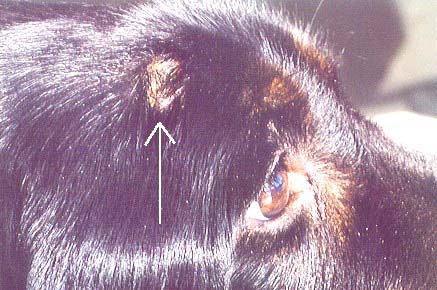
Clinical
Features - These depend on the stage of the disease. Fever,
coughing, dyspnea, anorexia, nasal discharge and progressive loss of condition
may be present. Subcutaneous purulent, ulcerative granulomas may also be seen.
As the disease spreads, signs reflecting involvement of various organs are
observed. Ocular involvement with anterior uveitis and subretinal effusion may
be seen. Without treatment the disseminated disease is invariably fatal.
Radiographs disclose swollen bronchial lymph nodes and nodular pulmonary
lesions.
Diagnosis -
- Cryptococcosis, nocardiosis, canine actinomycosis, coccidioidomycosis,
histoplasmosis, tuberculosis, chronic granulomatous infections of the skin due
to other agents and pneumonia due to other agents should be considered.
- Chest radiographs may suggest blastomycosis.
- Material is taken by transtracheal aspiration, transthoracic biopsy and
from granulomatous nodules or abscesses involving the skin. An ocular tap can
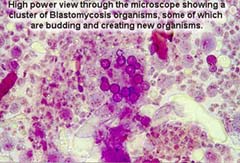
be used if the eye is thought to be involved. Examination of materials in wet
mounts for the characteristic thick-walled, single-budding yeasts.
Gram-stained smears are examined and culture at room and incubator temperature
(37ºC) on appropriate media.
- The finding of the typical organisms in sections of biopsies or affected
lung is highly diagnostic and is the usual means of diagnosis.
- Serum. Paired samples preferable.
- Paired samples are preferable. The agar gel immunodiffusion test for
antibody indicates a current or recent infection with a reliability of about
90 %.
- Definitive diagnosis depends on the isolation and identification of B.
dermatitidis; however, because it is very time-consuming it is not always
carried out.
Treatment -
- Itraconazole is the drug of choice; ketoconazole is an alternative.
Prolonged treatment, 2 - 3 months, is essential. The recurrence rate
may be as high as 20 %.
- A combination of amphotericin B with ketoconazole or itraconazole is used
for dogs with severe infections.
- In cases confined to the skin and subcutaneous tissue, lesions are removed
surgically.
Control - There are no practicable preventive
measures.
Public Health Significance -
Blastomycosis is
not considered contagious, but one should avoid contact with infectious
material. There are rare reports of humans acquiring the disease while
performing necropsies.
Blastomycosis (North American Blastomycosis)
Blastomycosis is
usually a severe disease, principally of the dog and human (rarely the cat and
other animals), caused by the fungus Blastomyces dermatitidis and
characterized by an infection that usually begins with the formation of
granulomatous nodules in the lungs.
The infection may be confined to the
lungs and regional lymph nodes or metastasize to produce the disseminated
disease with involvement of the skin, bone and other tissues and
organs.
Although there are usually numerous nodules in the lungs, in some
instances metastases may come from very limited pulmonary involvement.
Occasionally the infection is confined to lesions involving the skin and
subcutis. Such infections may persist for
months.
Etiology/Source - Blastomyces dermatitidis is
a soil-borne, dimorphic fungus. The mycelial phase occurs in nature and the
yeast form in vivo.
Distribution/Occurrence - It is probably
worldwide in distribution, although the number of cases reported outside of
North America is relatively small. The endemic area in the United States
includes the middle western, southeastern and Appalachian states. Although
single cases are most frequent, multiple cases have been reported in hunting
dogs.
Susceptibility - The disease occurs most frequently in
dogs; it is rare in cats. Humans are susceptible.
Mode of
Infection/Transmission - Inhalation of spores. Infrequently via
skin wounds leading to cutaneous lesions. Most often cutaneous lesions are
derived from pulmonary infection.
Incubation
Period/Course - . The incubation period is variable and may be as
long as several months. The course likewise is variable.
Clinical
Features - These depend on the stage of the disease. Fever,
coughing, dyspnea, anorexia, nasal discharge and progressive loss of condition
may be present. Subcutaneous purulent, ulcerative granulomas may also be seen.
As the disease spreads, signs reflecting involvement of various organs are
observed. Ocular involvement with anterior uveitis and subretinal effusion may
be seen. Without treatment the disseminated disease is invariably fatal.
Radiographs disclose swollen bronchial lymph nodes and nodular pulmonary
lesions.
Diagnosis -
- Cryptococcosis, nocardiosis, canine actinomycosis, coccidioidomycosis,
histoplasmosis, tuberculosis, chronic granulomatous infections of the skin due
to other agents and pneumonia due to other agents should be considered.
- Chest radiographs may suggest blastomycosis.
- Material is taken by transtracheal aspiration, transthoracic biopsy and
from granulomatous nodules or abscesses involving the skin. An ocular tap can
be used if the eye is thought to be involved. Examination of materials in wet
mounts for the characteristic thick-walled, single-budding yeasts.
Gram-stained smears are examined and culture at room and incubator temperature
(37ºC) on appropriate media.
- The finding of the typical organisms in sections of biopsies or affected
lung is highly diagnostic and is the usual means of diagnosis.
- Serum. Paired samples preferable.
- Paired samples are preferable. The agar gel immunodiffusion test for
antibody indicates a current or recent infection with a reliability of about
90 %.
- Definitive diagnosis depends on the isolation and identification of B.
dermatitidis; however, because it is very time-consuming it is not always
carried out.
Treatment -
- Itraconazole is the drug of choice; ketoconazole is an alternative.
Prolonged treatment, 2 - 3 months, is essential. The recurrence rate
may be as high as 20 %.
- A combination of amphotericin B with ketoconazole or itraconazole is used
for dogs with severe infections.
- In cases confined to the skin and subcutaneous tissue, lesions are removed
surgically.
Control - There are no practicable preventive
measures.
Public Health Significance -
Blastomycosis is
not considered contagious, but one should avoid contact with infectious
material. There are rare reports of humans acquiring the disease while
performing necropsies.
|