
Thomas J. Walsh Dennis M. Dixon
The clinical nomenclatures used for the mycoses are based on the (1) site of the infection, (2) route of acquisition of the pathogen, and (3) type of virulence exhibited by the fungus.
Mycoses are classified as superficial, cutaneous, subcutaneous, or systemic (deep) infections depending on the type and degree of tissue involvement and the host response to the pathogen.
Infecting fungi may be either exogenous or endogenous. Routes of entry for exogenous fungi include airborne, cutaneous or percutaneous. Endogenous infection involves colonization by a member of the normal flora or reactivation of a previous infection.
Primary pathogens can establish infections in normal hosts. Opportunistic pathogens cause disease in individuals with compromised host defense mechanisms.
The primary pathogens have relatively well-defined geographic ranges; the opportunistic fungi are ubiquitous.
Fungal infections or mycoses cause a wide range of diseases in humans. Mycoses range in extent from superficial infections involving the outer layer of the stratum corneum of the skin to disseminated infection involving the brain, heart, lungs, liver, spleen, and kidneys. The range of patients at risk for invasive fungal infections continues to expand beyond the normal host to encompass patients with the acquired immunodeficiency syndrome; those immunosuppressed due to therapy for cancer and organ transplantation, and those undergoing major surgical procedures. Each of these patient populations has a high risk of developing invasive fungal infections. As the population at risk continues to expand so also does the spectrum of opportunistic fungal pathogens infecting these patients also continue to increase. Many of the deeply invasive mycoses are difficult to diagnose early and often difficult to treat effectively. The development of new approaches to diagnosis and treatment of invasive fungal infections is the subject of intensive research.
Fungal infections may be classified according to the site of infection, route of acquisition, and type of virulence. When classified according to the site of infection, fungal infections are designated as superficial, cutaneous, subcutaneous, and deep (Fig. 75-1). Superficial mycoses are limited to the stratum corneum and essentially elicit no inflammation. Cutaneous infections involve the integument and its appendages, including hair and nails. Infection may involve the stratum corneum or deeper layers of the epidermis. Inflammation of the skin is elicited by the organism or its products. Subcutaneous mycoses include a range of different infections characterized by infection of the subcutaneous tissues usually at the point of traumatic inoculation. An inflammatory response develops in the subcutaneous tissue frequently with extension into the epidermis. Deep mycoses involve the lungs, abdominal viscera, bones and or central nervous system. The most common portals of entry are the respiratory tract, gastrointestinal tract, and blood vessels (Fig. 75-2).
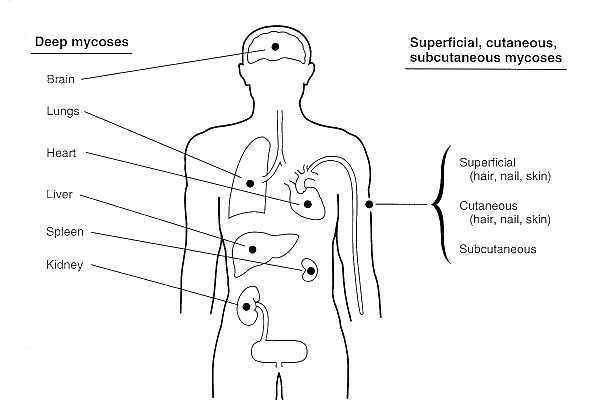
Figure 75-1 Principal tissue sites of deep mycoses in comparison to those of the superficial, cutaneous, and subcutaneous mycoses.
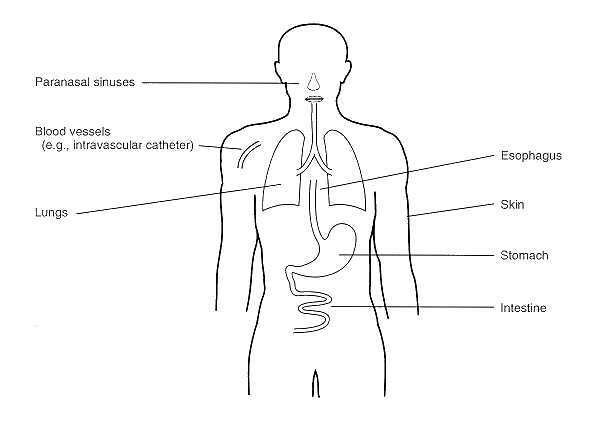
Figure 75-2 Portals of entry of pathogenic and opportunistic fungi causing deep mycoses.
When classified according to the route of acquisition, a fungal infection may be designated as exogenous or endogenous in origin. If classified as exogenous, an infecting organism may be transmitted by airborne, cutaneous, or percutaneous routes. An endogenously-acquired fungal infection may be acquired from colonization or reactivation of a fungus from a latent infection. Fungi may be classified also according to virulence, as primary pathogens or as opportunistic pathogens. A primary pathogen may establish infection in an immunologically normal host; whereas, an opportunistic pathogen requires some compromise of host defenses in order for infection to become established.
Superficial Mycoses include the following fungal infections and their etiological agent: black piedra (Piedraia hortae), white piedra (Trichosporon beigelii), pityriasis versicolor (Malassezia furfur), and tinea nigra (Phaeoannellomyces werneckii). Pityriasis versicolor is a common superficial mycosis, which is characterized by hypopigmentation or hyperpigmentation of skin of the neck, shoulders, chest, and back. Pityriasis versicolor is due to Malassezia furfur which involves only the superficial keratin layer. Black piedra is a superficial mycosis due to Piedraia hortae which is manifested by a small firm black nodule involving the hair shaft. By comparison, white piedra due to T beigelii is characterized by a soft, friable, beige nodule of the distal ends of hair shafts. Tinea nigra most typically presents as a brown to black silver nitrate-like stain on the palm of the hand or sole of the foot.
Cutaneous Mycoses may be classified as dermatophytoses or dermatomycoses. Dermatophytoses are caused by the agents of the genera Epidermophyton, Microsporum, and Trichophyton. Dermatomycoses are cutaneous infections due to other fungi, the most common of which are Candida spp. The dermatophytoses are characterized by an anatomic site-specificity according to genera. For example, Epidermophyton floccosum infects only skin and nails, but does not infect hair shafts and follicles. Whereas, Microsporum spp. infect hair and skin, but do not involve nails. Trichophyton spp. may infect hair, skin, and nails.
There are three general types of subcutaneous mycoses: chromoblastomycosis, mycetoma, and sporotrichosis. All appear to be caused by traumatic inoculation of the etiological fungi into the subcutaneous tissue. Chromoblastomycosis is a subcutaneous mycosis characterized by verrucoid lesions of the skin (usually of the lower extremities); histological examination reveals muriform cells (with perpendicular septations) or so-called "copper pennies" that are characteristic of this infection. Chromoblastomycosis is generally limited to the subcutaneous tissue with no involvement of bone, tendon, or muscle. By comparison, mycetoma is a suppurative and granulomatous subcutaneous mycosis, which is destructive of contiguous bone, tendon, and skeletal muscle. Mycetoma is characterized by the presence of draining sinus tracts from which small but grossly visible pigmented grains or granules are extruded. These grains are microcolonies of fungi causing the infection.
Chromoblastomycosis and mycetoma are caused by only certain fungi. The most common causes of chromoblastomycosis are Fonsecaea pedrosoi, Fonsecaea compacta, Cladosporium carionii, and Phialophora verrucosa. The causes of mycetoma are more diverse but can be classified as eumycotic and actinomycotic mycetoma. Within the United States, the most common agent of eumycotic mycetoma is Pseudallescheria boydii and the most common cause of actinomycotic mycetoma is Nocardia brasiliensis. Many of the fungi causing mycetoma are pigmented brown to black. These organisms are known as dematiaceous (melanized) fungi. The melanin pigment is deposited in the cell walls of these organisms. These fungi may produce a range of infections from superficial to subcutaneous to deep (visceral) infection characterized by the presence of dematiaceous hyphal and/or yeast-like cells in tissue. Such deep infections due to dematiaceous fungi are termed phaeohyphomycosis.
Sporotrichosis is the third general class of subcutaneous mycoses. This infection is due to Sporothrix schenckii and involves the subcutaneous tissue at the point of traumatic inoculation. The infection usually spreads along cutaneous lymphatic channels of the extremity involved.
Deep mycoses are caused by primary pathogenic and opportunistic fungal pathogens. The primary pathogenic fungi are able to establish infection in a normal host; whereas, opportunistic pathogens require a compromised host in order to establish infection (e.g., cancer, organ transplantation, surgery, and AIDS). The primary deep pathogens usually gain access to the host via the respiratory tract. Opportunistic fungi causing deep mycosis invade via the respiratory tract, alimentary tract, or intravascular devices.
The primary systemic fungal pathogens include Coccidioides immitis, Histoplasma capsulatum, Blastomyces dermatitidis, and Paracoccidioides brasiliensis. The opportunistic fungal pathogens include Cryptococcus neoformans, Candida spp., Aspergillus spp., Penicillium marneffei, the Zygomycetes, Trichosporon beigelii, and Fusarium spp.
Fungal dimorphism is the morphological and physiological conversion of certain fungi from one phenotype to another when such fungi change from one environment to another. Dimorphic fungi include C immitis, H capsulatum, B dermatitidis, P brasiliensis, P marneffei, and S schenckii, and certain opportunistic fungi such as Candida albicans and Penicillium marneffei. Various environmental host factors control fungal dimorphism. These factors include amino acids, temperature, carbohydrates, and trace elements (e.g. zinc). Among the primary pathogens and S schenckii, the morphological transformation is from a hyphal form to a yeast-like form (or spherule in the case of C immitis) in tissue (Fig. 75-3). However, the dimorphism of Candida albicans is somewhat different in that the organism transforms from a budding yeast-like structures (blastoconidia) to filamentous structures known as germ tubes (Fig. 75-4). Other filamentous structures may later develop as pseudohyphae and hyphae. Penicillium marneffei is unique in being the only Penicillium species pathogenic to humans. It undergoes dimorphic conversion in vivo to transversely dividing sausage-shaped cells.
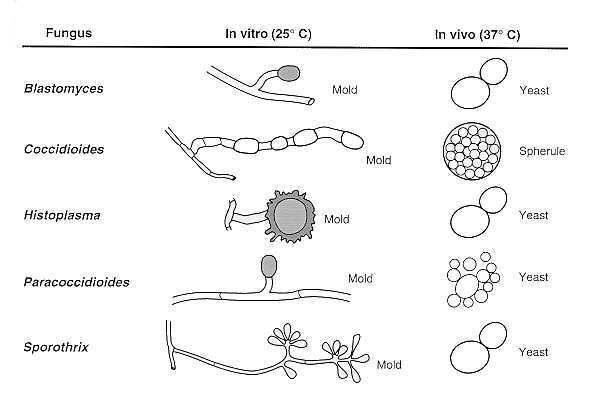
Figure 75-3 Diagrammatic representation of the saprophytic and invasive tissue forms of pathogenic fungi.
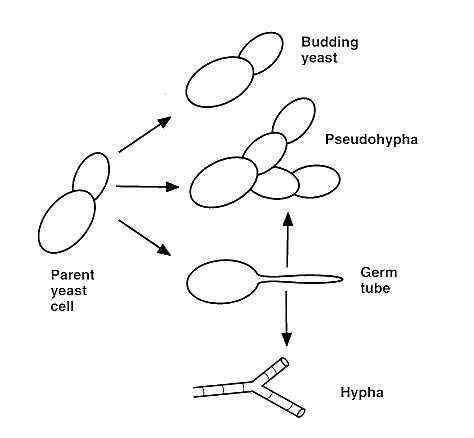
Figure 75-4 Germination of Candida albicans.
Most cases of primary deep mycoses are asymptomatic or clinically mild infections occurring in normal patients living or traveling in endemic areas. However, patients exposed to a high inoculum of organisms or those with altered host defenses may suffer life-threatening progression or reactivation of latent foci of infection.
The arthroconidia of C immitis are inhaled and convert in the lung to spherules. Most cases of coccidioidomycosis are clinically occult or mild infections in patients who inhale infective arthroconidia. However, some patients have progressive pulmonary infection and also may suffer dissemination to the brain, bone, and other sites. Coccidioides meningitis is a life-threatening infection requiring lifelong treatment.
Histoplasmosis is a primary pulmonary infection resulting from inhalation of conidia of Histoplasma capsulatum which convert in vivo into the blastoconidial (budding yeast) form.
Dissemination to the hilar and mediastinal lymph nodes, spleen, liver, bone marrow, and brain may be life-threatening in infants and other immunocompromised patients. Histoplasmosis (like tuberculosis) is characterized by intracellular growth of the pathogen in macrophages and a granulomatous reaction in tissue. These granulomatous foci may reactivate and cause dissemination of fungi to other tissues. These patterns of primary infection and reactivation are similar to those of Mycobacterium tuberculosis (see Chapter 33). Histoplasmosis also may be associated with a chronic inflammatory process known as fibrosing mediastinitis, where scar tissue (formed in response to H capsulatum) encroaches on vital structures in the mediastinum.
Blastomycosis, similar to histoplasmosis, is a primary pulmonary infection resulting from inhalation of conidia from the mycelial phase of Blastomyces dermatitidis which convert in vivo to the parasitic yeast phase. Blastomycosis (due to B dermatitidis) in the blastoconidial phase also causes a primary pulmonary infection. The organism elicits a granulomatous reaction often associated with a marked fibrotic reaction. The clinical pattern of pulmonary blastomycosis is one of chronic pneumonia. Dissemination occurs most commonly to the skin, bone, and, in males, prostate.
Candidiasis. Candidiasis (due to C albicans and other Candida spp.) is the most common opportunistic fungal infection. Candida albicans is the most common cause of candidiasis. Candidiasis may be classified as superficial or deep. Superficial candidiasis may involve the epidermal and mucosal surfaces, including those of the oral cavity, pharynx, esophagus, intestines, urinary bladder, and vagina. The alimentary tract and intravascular catheters are the major portals of entry for deep (or visceral) candidiasis. The kidneys, liver, spleen, brain, eyes, heart, and other tissues are the major organ sites involved in deep or visceral candidiasis. The principal risk factors predisposing to deeply invasive candidiasis are protracted courses of broad spectrum antibiotics, cytotoxic chemotherapy, corticosteroids, and vascular catheters.
Aspergillosis. Invasive aspergillosis most frequently involves the lungs and paranasal sinuses. This fungus may disseminate from the lungs to involve the brain, kidneys, liver, heart, and bones. The main portal of entry for aspergillosis is the respiratory tract, however, injuries to the skin may also introduce the organism into susceptible hosts. Quantitative and functional defects in circulating neutrophils are key risk factors for development of invasive aspergillosis. For example, neutropenia due to cytotoxic chemotherapy and systemic corticosteroids are common predisposing factors for invasive aspergillosis.
Zygomycosis. Zygomycosis due to Rhizopus, Rhizomucor, Absidia, Mucor species, or other members of the class of Zygomycetes, also causes invasive sinopulmonary infections. An especially life-threatening form of zygomycosis (also known as mucormycosis), is known as the rhinocerebral syndrome, which occurs in diabetics with ketoacidosis. In addition to diabetic ketoacidosis, neutropenia and corticosteroids are other major risk factors for zygomycosis. Aspergillus spp and the Zygomycetes have a strong propensity for invading blood vessels.
Cryptococcosis. Cryptococcosis is most typically an opportunistic fungal infection that most frequently causes pneumonia and/or meningitis. Defective cellular immunity, especially that associated with the acquired immune deficiency syndrome, is the most common risk factor for developing cryptococcosis.
Phaeohyphomycosis. Phaeohyphomycosis is an infection by brown to black pigmented fungi of the cutaneous, superficial, and deep tissues, especially brain. These infections are uncommon, life-threatening, and occur in various immunocompromised states.
Hyalohyphomycosis. Hyalohyphomycosis is an opportunistic fungal infection caused by any of a variety of normally saprophytic fungi with hyaline hyphal elements. For example, Fusarium spp. infect neutropenic patients to cause pneumonia, fungemia, and disseminated infection with cutaneous lesions.
The epidemiology of dimorphic primary pathogens may be contrasted with that of the opportunistic fungal pathogens.
The primary pathogens have a relatively well-defined geographic range of endemic infection in immunocompromised hosts. By comparison, the opportunistic fungi (e.g. Aspergillus spp.) are ubiquitously distributed with the frequency of infection being dependent upon a population of immunocompromised hosts. Penicillium marneffei, an opportunistic pathogen, appears to be geographically restricted to the East Asia, particularly Thailand and China.
Control and Treatment
Hospital-acquired fungal infections may be reduced by maintaining the lowest possible concentration of fungal spores in the ambient air of the institution. Ideally, a "spore-free" environment should be sought. Antifungal therapy, which is reviewed in depth elsewhere, is an area of intense investigation (See Chapter 76). New antifungal compounds will hopefully improve the efficacy and reduce toxicity of treatment of invasive fungal infections.
Bodey GP (ed.): Candidiasis. 2nd ed. Raven Press. pp. 1, 1992
Dupont B, Denning DW, Marriott D, Sugar A, Viviani MA, Sirisanthana T, Elewski,, BE (eds.): Cutaneous Fungal Infections. Topics in Clinical Dermatology. Igaku-Shoin. pp. 1, 1992
Kwon-Chung KJ and Bennett JE: Medical Mycology. Philadelphia: Lea & Febiger, 1992
Matsumoto T, Ajello L, Matsuda T, Szaniszlo PJ, and Walsh TJ: Developments in phaeohyphomycosis and hyalohyphomycosis. J Med Vet Mycology. 32 (suppl 1):329, 1994
McGinnis MR: Laboratory Handbook of Medical Mycology. New York: Academic Press, 1980
Mycoses in AIDS patients. J Med Vet Mycol; 32 Suppl 1:65, 1994
Odds FC, Arai T, DiSalvo AF, Evans EGV, Hay RJ, Randhawa HS, Rinaldi MG, Walsh TJ: Nomenclature of fungal diseases. J Med Vet Mycol. 30:1, 1992
Odds FC: Candida and Candidosis. A Review and Bibliography. 2nd ed. Philadelphia: Bailliere Tindall; 1988
Pappagianis D: Coccidioidomycosis. Semin Dermatol. 12:301, 1993
Pfaller MA and Fromtling RA (eds): Mycology. In P Murray, EJ Baron, MA Pfaller, FC
Tenover, RH Yolken (eds). Manual of Clinical Microbiology. 6th. ed. American Society for Microbiology. Washington, D.C. pp. 699, 1994
Rinaldi MG, Dixon DM (eds.). The evolving etiologies of invasive mycoses. Infect Dis Clin Pract. 3 (suppl):S47, 1994
Rippon JW: Medical Mycology. The Pathogenic Fungi and The Pathogenic Actinomycetes. 3rd ed. Philadelphia: WB Saunders Co; 1988
Sarosi G and Davies S: Fungal Diseases of the Lung, 2nd. ed. Raven Press, New York, NY; pp. 1, 1993
Sternberg S: The emerging fungal threat. Science. 266: 1632, 1995
Viviani MA, Hill JO, Dixon DM: Penicillium marneffei: dimorphism and treatment. p.413-423. In Vanden Bossche, H., Odds, FC, and Kerridge, D. (eds) Dimorphic Fungi in biology and medicine. Plenum Press. New York, 1993
Walsh TJ, DePauw B, Anaissie E, Martino P: Recent advances in the epidemiology, prevention, and treatment of invasive fungal infections in neutropenic patients. J Med Vet Mycol. 32 (Supplement 1): 33, 1995
Walsh TJ, Gonzalez C, Lyman CA, Chanock S, and Pizzo PA: Invasive fungal infections in children: recent advances in diagnosis and treatment. Advances in Pediatr Infect Dis. 11: 175, 1995
Walsh TJ, Pizzo PA: Nosocomial fungal infections. Ann Rev Microbiol. 42:517, 1988.